Source: [4]
Ethiopian Demography and Health
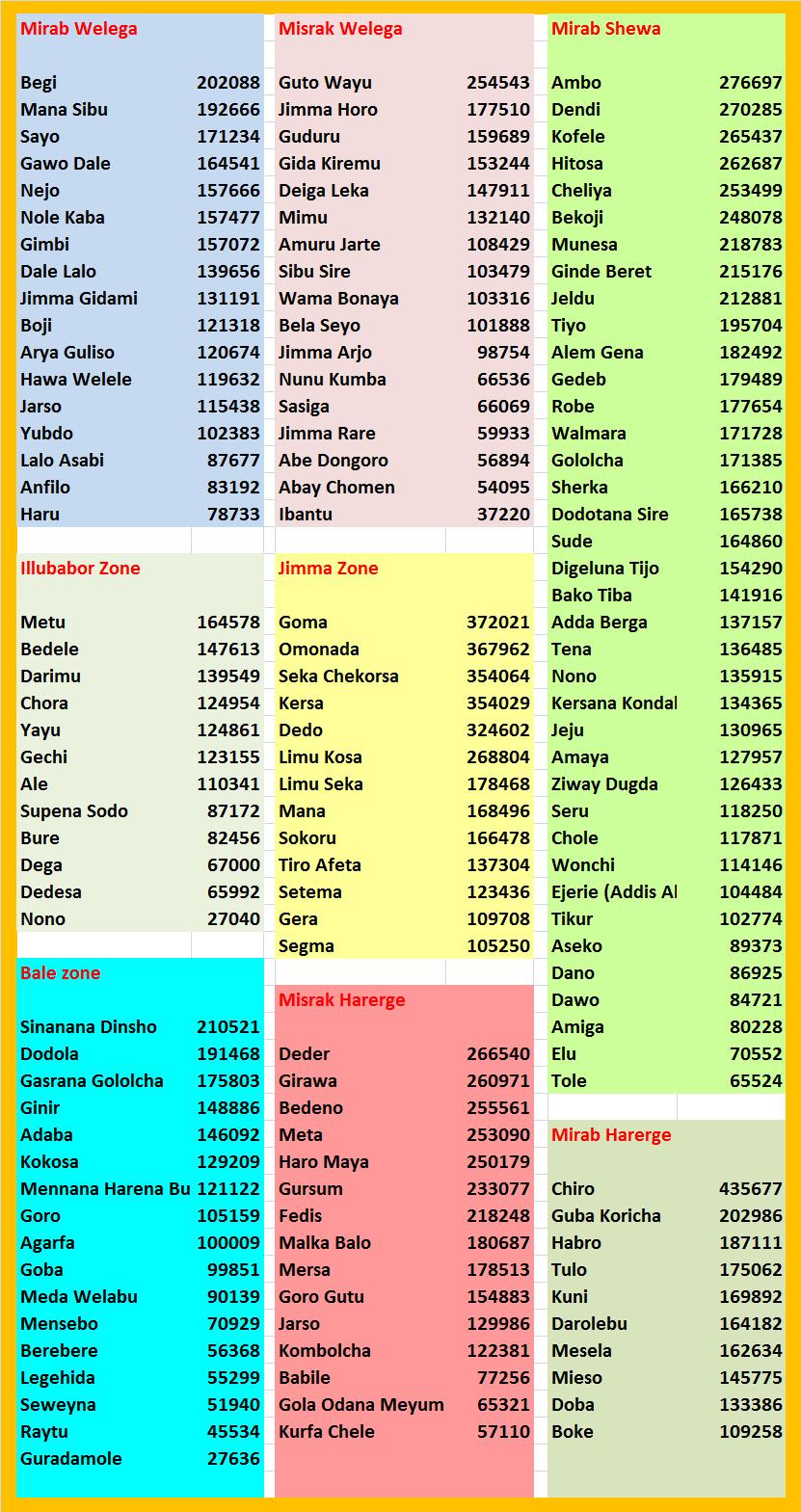
With 353,690 square kilometers of land area (32% of the country), Oromiya represents the largest regional State [1]. The CSA estimate of 28,067,000 people for July 2008 [2] and 38 million in Mid 2018 indicates that its population size is also the largest. The Oromo represent the majority ethnic group in Oromiya (85%), and in the country at large. Nearly 4 million are residents of urban areas giving an urbanization rate of 13.8% - slightly below the national average. Their percentage proportion has been estimated variously at 35% and higher, up to 40% of the country’s total although the higher figure seems to represent the real proportion. Administratively, Oromiya is divided into 17 zones, 245 Weredas, and 36 town administrations with 6500 kebele subdivisions (see map below).
There is an apparent unanimity among authors, that the Oromo had not been part of present-day Ethiopia’s settled landscape prior to the 1550s. In the absence of scientific research and accurate historical accounting of their beginnings, the Oromo have often been described as “migrants” who arrived in Ethiopia proper from its southern-most reaches in mid-16th century, and settled amicably among all groups whose lands they had “appropriated”. Other labels used in place of migration include invasion, plunder, onslaught, conquest, etc. The source below also described them as aliens, and charactezed their early roles as destructive:
“Oromo, settled in far southern Ethiopia, were an egalitarian pastoral people divided into a number of competing segments or groups but sharing a type of age-set system of social organization called the gada system, which was ideally suited for warfare. Their predilection toward warfare, apparently combined with an expanding population of both people and cattle, led to a long-term predatory expansion at the expense of their neighbors after about 1550. Unlike the highland Christians or on occasion the lowland Muslims, the Oromo were not concerned with establishing an empire or imposing a religious system. In a series of massive but uncoordinated movements during the second half of the sixteenth century, they penetrated much of the southern and northern highlands as well as the lowlands to the east, affecting Christians and Muslims equally….. The effect of the Oromo migrations was to leave the Ethiopian state fragmented and much reduced in size, with an alien population in its midst.” [3]
The Oromiya regional State extends from the western end of the country in western Wellega to the eastern parts of eastern Harrarge from 34°E latitude to 43°E. It’s southnorth expanse runs from 4⅔°North to 10⅔°North latitude. Topographically and climatically the region is diverse with sharp contrasts noted for the mid portion Oromiya formed by the Great Rift Valley system that divides the regional State roughly into a western third and eastern two-thirds.
“Oromia is a region of great physiographic diversity. Its landscape includes high and rugged mountain ranges, undulating plateaus, panoramic gorges and deep incised river valleys, and rolling plains. Rising from less than 500 meters above sea level to high ranges that culminate into Mt. Batu (4607 m) - the highest peak of the region. Oromia is endowed with varied relief features which inturn accentuate varied and amiable climatic condition and other rich natural resource bases".
"Oromia is a remnant part of the high and extensive Afro-Arabian plateau formed from continued uplift, rifting and subsequent volcanic piles. High relief of over 1500m is dominant. The climatic types prevailing in the region may be grouped into 3 major categories: the dry climate, tropical rainy climate and temperate rainy climate. The dry climate is characterized by poor sparse vegetation with annual mean temperature of [27 degree C to 39 degree C], and mean annual rainfall of less than 450 mm. The hot semi-arid climate mean annual temperature varies between [18 degree C and 27 degree C]. It has a mean annual rainfall of 410-820 mm with noticeable variability from year to year. Highlands of Oromiya experience temperate climate of moderate temperature, (mean temperature of the coolest month is less than [18 degree C]) and ample precipitation (1200-2000mm)” ….[Awash, Wabe-Shebele, Genale, Gibe, Baro, Dedessa and Guder are major rivers in the region. River Awash, which is the longest river inside Ethiopia is a source of great agroindustrial and hydroelectric power. The crator lakes Green lake (true to its name), Bishoftu, Kuriftu, Bishoftu-Gudo, Hora-Kilole, Horsa Arsedi, and the rift-valley lakes Ziway, Abiyata, Shala, and Langano are found in this region. They have immense potential for recreation and fishery development. …There are around 800 bird species and more than 100 wild animals in the region. Endemic wild animals such as the mountain Nyala, the Semien Red Fox and Menelik Bushbuck inhabit the Bale mountains national park".
"The Awash National Park, the oldest and most developed game reserve of its kind in Ethiopia, consists most of the East African plain games except Giraffe and Buffalo. It is home to the Oryx, Kudu, Caracal, Aardavark, Colobus Monkey, Green Monkeys, Baboons, Leopard, Klipspringer, Hippo, Seemering's Gazelle, Grevy's Zebra and Cheetah".
"The Awash National Park is also a natural sanctuary of numerous bird-species, some of which include Limburger, Wattle Crane, Angur Buzzard, Verreaux Eagle and long eared owls. Water Fowls, Shore Birds and the colorful Ruddy Shelled Duck as well as the endemic Blue-winged Goose are common in the marshy areas of the park”. [1].
An online resource developed by the regional government [4] makes a brief mention of the 30 major forest areas distributed within the various ago-ecological zones, the increasing pressure on land resources due to increasing human and animal populations, the gradual depletion of vegetation and soil resources, the increasing demand for agricultural and grazing land as well as for more fuel and construction materials, and the resulting overall environmental damage. Its detailed reports about the region include the following:
Agriculture
“Generally, by virtue of relatively abundant rainfall, suitable soils and other agricultural potentialities, Oromia remains the major crop producing region in the country. Accordingly, Oromia has accounted for 49% of major food crops production 50.8% of cereals, 37% of pulses and 43.56% of oil crops production of total peasant holdings of the country in 1994 E.C. production year (CSA, 1994 E.C).”
On the negative side “…..crop production is characterized by smallholding of just over a hectare and limited use of input such as fertilizers, pesticides, improved seeds and implements. Moreover, heavy dependence on rain fed (limited or no use of irrigation) cultivation practice is another essential feature of smallholding peasant farming in Oromia. Thus, yield per hectare has remained extremely low and growth in production is sluggish with the an average yield of 12.49 quintals per hectare, which is by far below the potential of fifty quintals for wheat and up to eighty quintals for maize with the application of package of inputs.”
“Despite the fact that the extension services on the use of fertilizer has started long ago, the level of utilization of this technology by the farmers is still very low. The average fertilizer use during the reference period was below 35 kg per hectare (assuming a standard of 100 kg/ha.) which is the lowest in the world , while that of improved seed is also very low at an average of 1.7 kg per hectare. Generally, only 45% and 3.7% of the total land under cultivation in the region were covered by fertilizer and improved seeds respectively implying low level of input use, contributing to low productivity among other factors. The situation is further aggravated by insufficient supply of other agricultural technologies such as chemicals and farm implements.”
“Coffee is the major source of foreign exchange for the country accounting for 50–60% of total exports. Oromia accounted for 77.6 percent of coffee plantation as per the 1988–1992 [Ethiopian Calendar] plan evaluation report and delivered annually about 68% of coffee destined for foreign market. Similarly, out of 53 districts known for Coffee production in the country 42 (79%) are found in Oromia showing the tremendous resource base the region is endowed with.”
“….the land covered by coffee plantation in 1987 and 1992 was estimated to be 209 and 260 thousand hectares respectively, while the annual production for the same years was estimated at 901 and 1190 thousand quintals. The average annual growth rate over these years was 4.47% for land and 5.7% for production. Similarly, the average annual delivery of coffee to the central coffee market was about 835.46 thousand quintals with production range between 662 and 942 thousand quintals in the year 1988 and 1990.”
“One of the reasons for low agricultural performance and low income levels in the region is the tendency of traditional focus which is in favor of cereal production in spite of the extremely high agro-ecologic diversities and the resource potentials for production and diversifications into relatively high yielding and high income generating horticultural crops (vegetables and root crops), fruits, flowers, spices and chat. Cereals crop development has been receiving almost the entire attention both in terms of extension interventions and resource allocation in the past years possibly from the stand point of attaining food self-sufficiency and lack of market.”
Oromiya also has its share of the regular disasters, mostly natural, but also man-made, such as food shortages, disease outbreaks, flooding, and droughts.
“Every year drought affects more than 500,000 people especially in Borena Zone. In 2006 Flood has affected 21,900 people and has displaced 9,052 people. In Oromiya regional state initially Acute Watery Diarrhea (AWD) out break cases were identified in West Arsi, Arsi Negle Woreda Danshe village on June 22/06/06. Currently 63 districts (woredas) in 8 zones out of 23 are affected in Oromiya Region. A total of 26,427 AWD cases and 286 deaths were reported up to date (CFR: 1.1%). In 2006 polio and measles out-breaks were also reported from Oromiya Region. Additionally Avian Influenza and Rift Valley fever remain other health threats for Oromiya Regional State.” [5]
Health Care:
A recent WHO emergency mission reported the existence of “29 hospitals, 192 health centers, 895 health stations and 1070 health posts, owned by government, other Gov. and NGOs”. It also estimated the number of health professionals at about 8,172 trained partly at one of the seven health science colleges and another 18 centers providing health training's for midlevel health professionals and extension workers. “The potential health service coverage is 70.5% and the health service utilization is 27%” [5] There is an urban-rural difference in source of water and method of collection. “The urban dwellers are mainly using tap water, while the rural communities are using water from different sources mainly from rivers”. [5].
“The water supply coverage of the region is 13.6 % which is very low, and the rural population of the region has limited access to improved water supply service. This is worse even for sanitation coverage, which is only 7.6 %. The number of latrines constructed in the rural areas is very low and the majority of the people are not aware of personal hygiene and environmental sanitation. The communities are practicing poor-disposal of excreta, unhygienic handling of food and utensils and poor domestic waste disposal including animal wastes” [6]
Education:
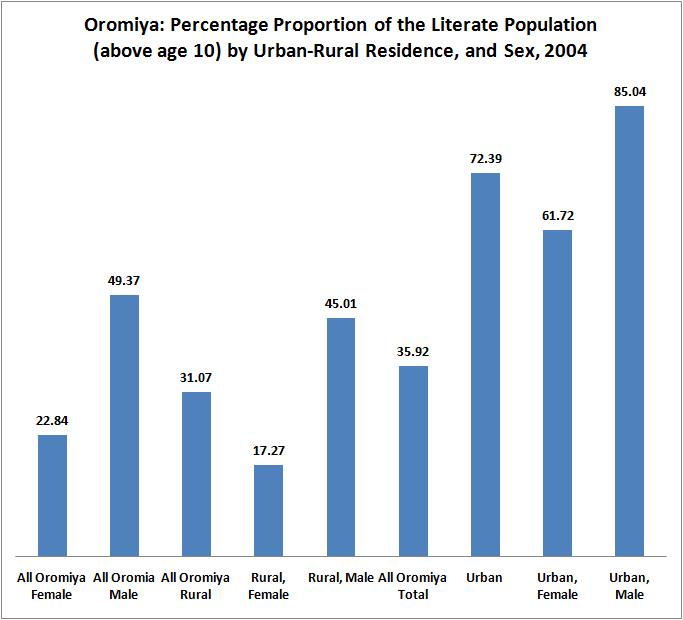
Literacy rates are significantly higher among Oromo males than females (see the graph below). While 36 percent of all residents of Oromiya were literate in the year 2004 the rural rate was much lower (31%) than the overall urban rate (72.4). There is a significant difference in the male-female rates too, with the overall female rate (22.8%) at less than half the males rate (49.4%). Only 17% of the female residents of rural Oromiya (85% of them ethnic Oromos) were literate with all of its implication for their way of life, health, child bearing and rearing, maternal and child nutrition, as well as disease prevention. It would be justified to expect a prevailing high fertility and morbidity regime. This will be investigated in the forthcoming paragraphs. On the bright side, nearly two-thirds of urban women are literate.
Source: [2]
Population Distribution
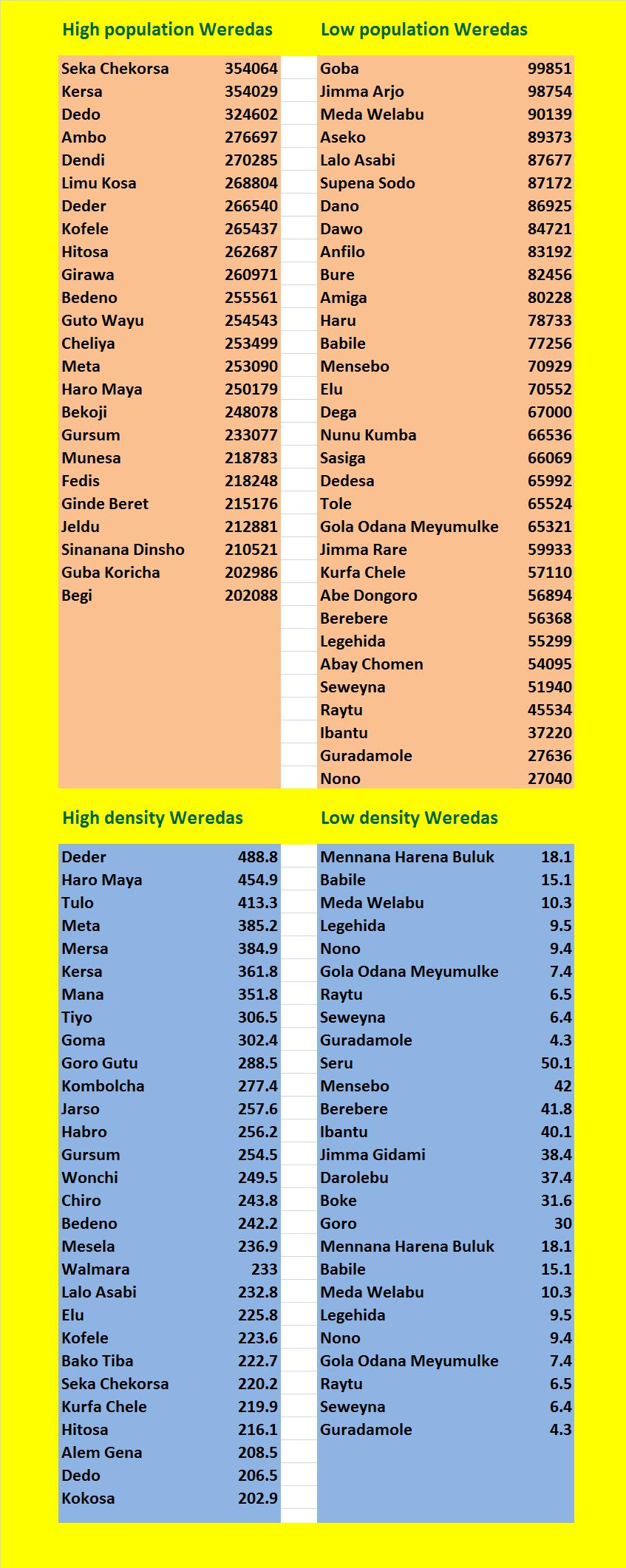
The table below shows Weredas in Oromiya with the highest and lowest populations in July 2008. Seka chekorsa in Illubabor has the highest population of any Wereda in Oromiya followed closely by Kersa (also in Illubabor) with nearly identical population size. Dedo, in the same administrative zone has the third largest population and is the only other Wereda with a population of over three hundred thousand. With a population less than a tenth of the most populated Weredas Nono (Mirab Shewa) and Guaradamole (Bale zone) represent the least populated Weredas in Oromiya. Twenty three Weredas have a population of 200,000 or more, and 31 Weredas have a population of less than 100,000.
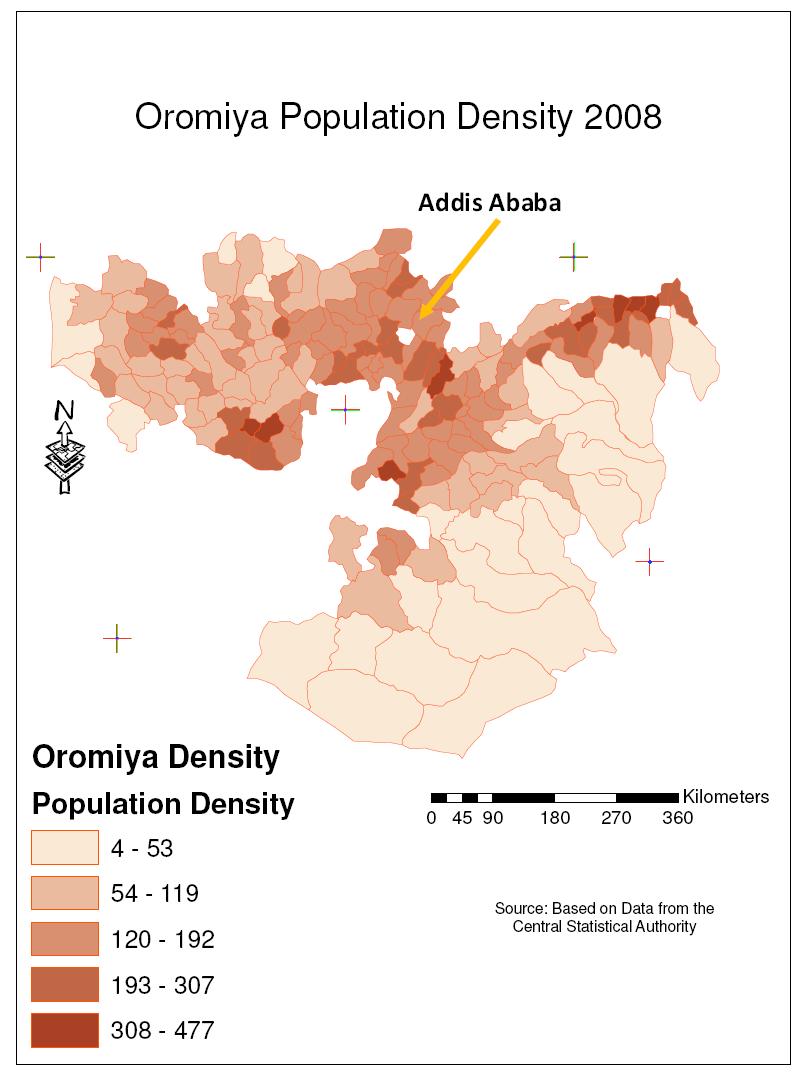
The lower half of the table below ranks Wereda's in Oromiya in decreasing order of density. Weredas with the highest most densities (over 200 persons per square meter) are shown on the left, and those with lowest densities - below 20 persons per square kilometers (less than a tenth of the densest Weredas) - are shown on the right. Deder (Misrak Harerge) is the highest density Wereda in Oromiya followed by Haro Maya (also in Misrak Harerge). Tulo (Mirab Haregrge) is a close third, and is the only other Wereda in Oromiya with a population density of over 400 persons per square kilometers. Weredas with the lowest densities (below 20) are listed on the right. Guaradamole (Bale zone) has the least density in Oromia. Other Weredas in Oromiya with the lowest densities of less than 10 persons per square kilometers include Seweyena, Raytu, Gola Odana Meyumulke, Nono, and Legehida (see the density map below the table).
References:
1. http://www.ethiopar.net/type/English/basinfo/infoormy.htm#area
http://www.ethiopar.net/type/English/basinfo/infoormy.htm#area
2.http://www.csa.gov.et/text_files/national_statistics.htm
3.http://countrystudies.us/ethiopia/11.htm
4.http://www.oromiagov.org/CropProduction.asp
5.WHO Emergency Humanitarian Action (EHA), Ethiopia Programme. Report on Field Trip to Provide
Technical Support in Emergency Preparedness and Response to Oromiya Regional State. 2007.
6.Central Statistical Authority, Statistical Abstract. 2001 pp. 26-45
7.Ethiopia Demographic and Health Survey 2005 Central Statistical Agency, Addis Ababa, Ethiopia ,
RC Macro, Calverton, Maryland, USA, September 2006
8.http://www.prb.org
9.http://www.medicineau.net.au/clinical/womenshealth/Antenatal.html

Source: http://www.ocha-eth.org/Maps/downloadables/OROMIYA.pdf
The Table below shows the population sizes of all Weredas in Oromiya by Zone and by decreasing order of population sizes. The population estimates are for July 2008
Socio Economic Characteristics:
Family structure:
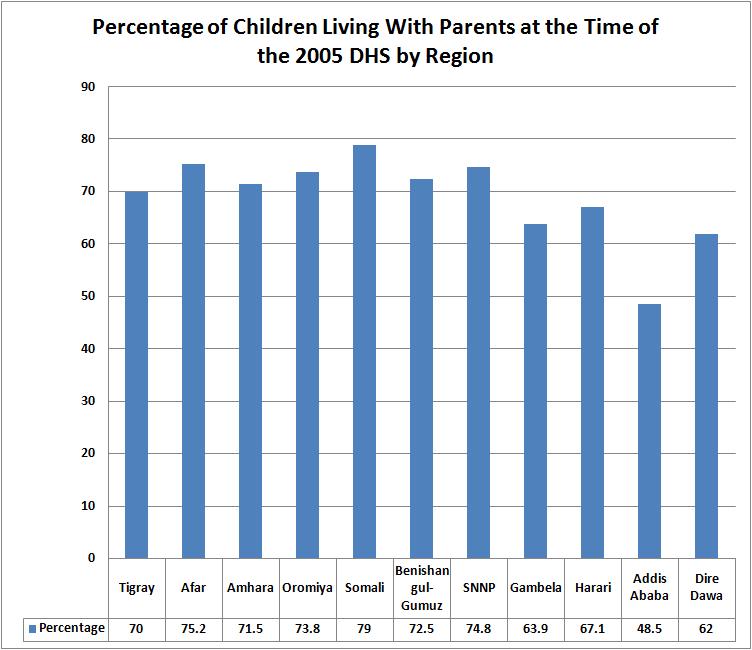
Oromiya has the fourth largest percentage of children living with both parents. For reasons that may or may not lend themselves to readily available explanations, Somali has the highest such percentage. Is this due to the age-old nomadic life style forcing families to stay together for security and survival? The fact that Afar is at number two (see graph below) might appear to lend credence to this assertion but the validity of this argument remains suspect given that the population in the number 3 region - SNNP - is not predominantly nomadic. All of the graphs below are based on data from the 2005 DHS [7].
Educational characteristics of respondents
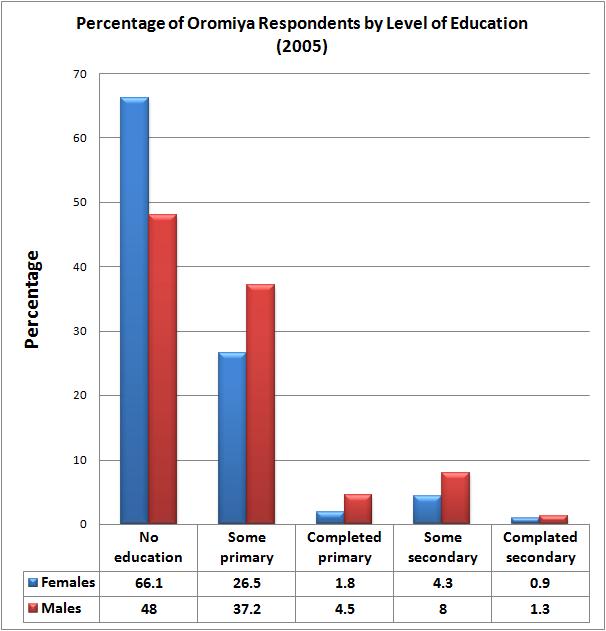
The gender difference in educational attainment is very clear from the graph below. Even though this is hardly unique to Oromiya, there are nearly 40 percent more females above the age of six with no education than men. Just over a quarter of females have completed some primary schooling while more than a third of the men have. Very few have gone beyond this stage, with only 4.5% of males and 1.8% of females reporting themselves as having completed primary school; 4.3 and 8 percent of females and males had reached the secondary level respectively, and even a lower percentage than that had completed it.
Family "wealth"
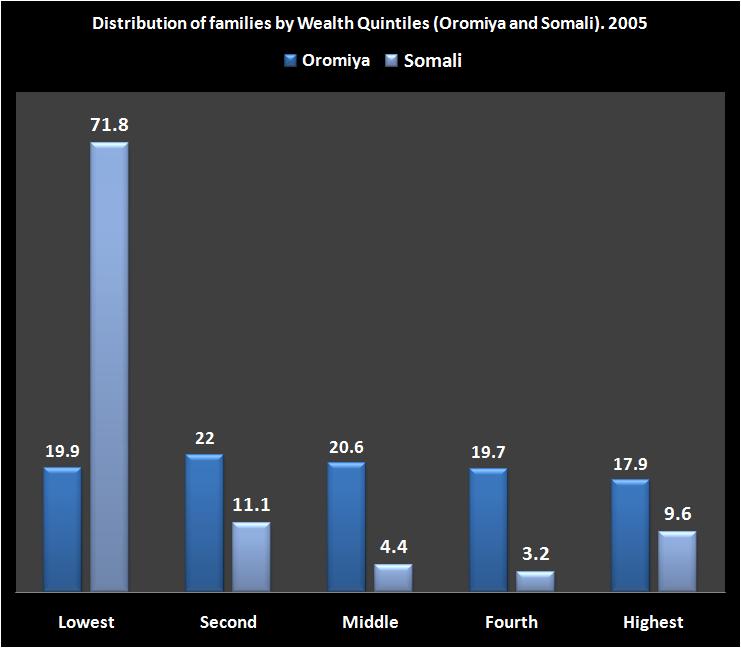
The graph below compares families in various wealth quintiles. Somali is chosen to provide a contrast as a region the is next door to Oromiya but with a population predominantly engaged in economic activities in stark contrast to the majority of Oromiya residents. The later are mostly settled agriculturalists while the Somalis are primarily nomadic herders. The graph is a powerful testimony that with nearly three-quarters of Somalis in the lowest wealth quintile nomadic herding is much less likely to lead to a descent standard of living (even by Ethiopian standards) than settled agriculture. Less than a fifth of Oromiya residents are in this category. In addition, nearly five times as many, and six times as many families in Oromiya than Somali are in the middle and fourth quintiles respectively.
Exposure to media
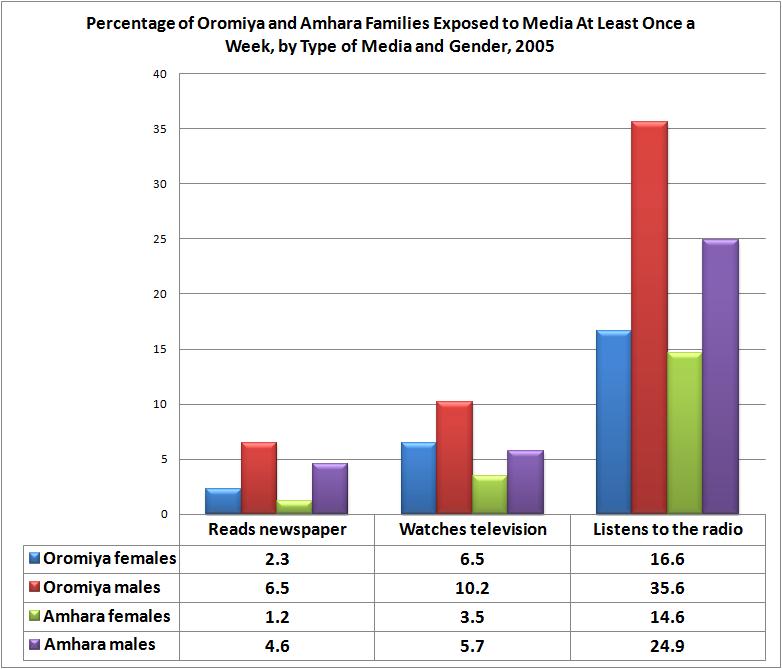
A neighboring administrative State - Amhara - is added (see graph below) to offer a comparative evaluation of how informed the populace is in the biggest and second biggest regions of the country. Exposure to media can greatly influence social and economic progress or lack thereof. A highly informed population is better prepared and capable of knowing about and adopting new innovations be it economic, or social, or demographic. For example, a woman accessing a daily dose of health information from the print or broadcast media is better able to seek preventive and treatment regimes that could help protect her children from ill health and its debilitating impacts.
Of the four groups represented below, Amhara women are the least informed (least exposed to media), and Oromiya men are the best informed both in comparison to Oromiya females and their Amhara male compatriots. Twice as many males than females in Oromiya listen to the radio at least once a week although (presumably) they live in the same household. This might be an indirect indicator of the amount of leisure time available to the two genders with males enjoying the lion's share of it. Not surprisingly, the lowest percentage is noted in the "reads news paper" category indicating both the lack of access to print media, as well as the very low level of literacy, especially among females. The low percentage of TV viewing is almost certainly a reflection of the higher cost of television sets and its restriction to a limited number of urban viewers. The radio is the cheapest and most accessible medium.
Demographic Characteristics:
Fertility
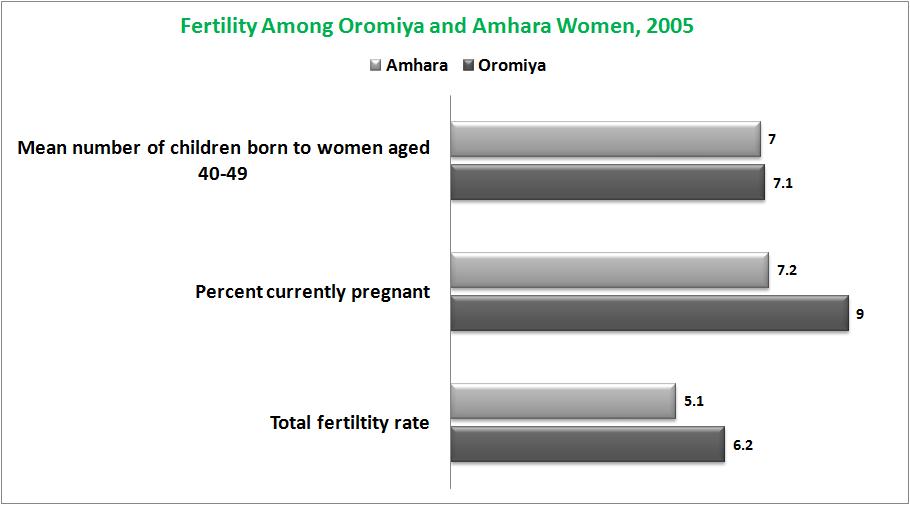
The Oromiya region has the highest fertility in the country. The total fertility rates (see graph below) indicate that Oromiya women currently in their reproductive years will have one child more than Amhara women at the conclusion of their reproductive performance. Since the total fertility rate - TFR - is calculated on the basis of whether or not women had a birth in the 12 months prior to the 2005 survey the rates are subject to change and sensitive to errors resulting from memory lapse and intentional concealment of births that have taken place. Comparison of the number of children ever born - CEB - to women at the conclusion of their reproductive years (age 40-49) proves that the Oromiya-Amahara fertility difference resulted from a recent decline in fertility in the Amhara region. The CEB numbers show the cumulative fertility experience stretching several decades, and show that, in the past, Oromiya and Amhara women reproduced at rates that are much less dissimilar. The difference in percentages of Amhara and Oromiya women who reported themselves to be currently pregnant also proves that current fertility is definitely lower in Ahmara than in Oromiya.
DETERMINANTS OF FERTILITY
Birth interval
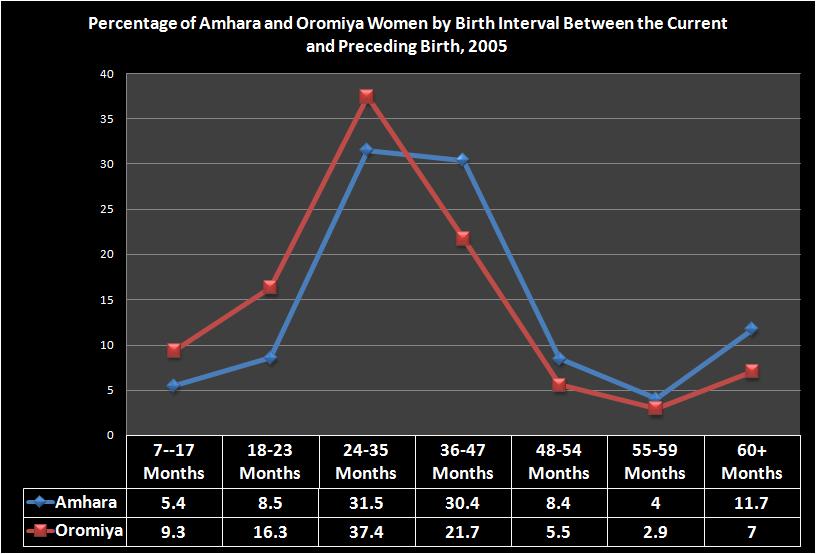
In the absence of contraception and continuous exposure through intercourse, the shorter the interval of time between births the more children a woman would bear during her reproductive life time. Here too, there is a clear contrast between women in Oromiya and Amhara with the numbers suggesting that the fertility difference is real, and not an artifact of data errors. The median birth interval among Amhara women between the "current birth" and the preceding birth is 37 months. Among Oromiya women it is 31 years. More than half of Amhara women (55%) had waited three years or more; just over a third (37%) of Oromiya women waited that long (see graph below). The left and right halves of the graph tell contrasting stories with higher percentage of Oromiya women represented in the lower interval classes (left half) and a higher percentage of Amhara women in the higher interval classes (the right half).
Age at marriage
Continued comparison between Oromiya and Amhara women (see graph below) will help unravel the mysteries behind fertility differences between different groups in Ethiopia whether small or large. One such factor is age at marriage. Given the cultural restrictions against sex before marriage, age at marriage becomes one of the major determinants of exposure to pregnancy and child birth. The graph below shows a lower median age at marriage for Amhara than Oromiya women, which would suggest a higher fertility among Amhara women. But this is counteracted by the negative fertility impacts among Amhara women, of such other influences as longer birth intervals, longer breastfeeding, instability of marriage, etc. The current cohorts of 25-29, 30-34, 35-39, 40-44, and 45-49-year-old Amhara women married at least a year younger than their counterparts in Oromiya. The gap is long enough to result in a one-child "fertility advantage" for Amhara women, who actually have a one-child "fertility disadvantage" due to other intervening factors which have limited reproductivity among Amhara women.
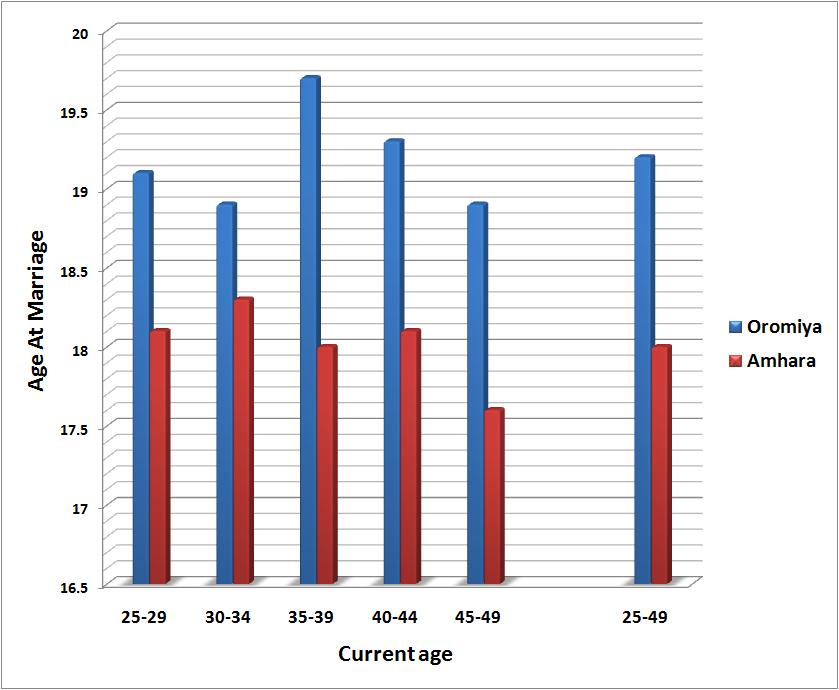
Median Age at Marriage Among Amhara and Oromiya Women by Current Age Group (2005)
Fertility in the early years of child bearing (teenage fertility)
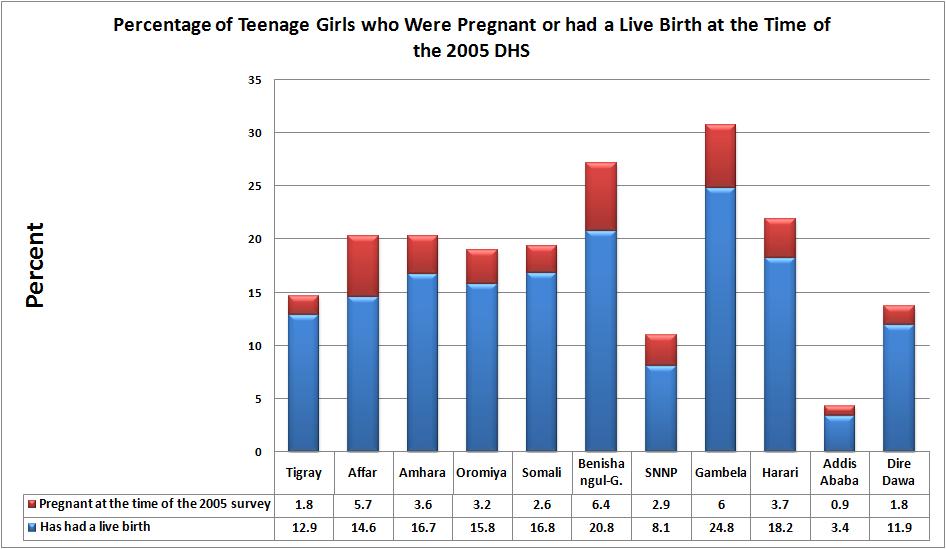
In developed countries teenage pregnancy is considered one of the social ills society should confront due to its detrimental effects on the educational and career prospects of young mothers. In Ethiopia, however, school attendance rates are so low among girls especially in rural areas where over four-fifths of the women live, and cultural dictates requiring virginity at the time of marriage are so strong, early marriage, pregnancy, and child-bearing among teens is not considered as a social ill at all. Oromiya's percentages of teenage girls in the two categories (pregnant or with a child - see graph below) is not high. It is roughly the same as the national average which is weighed down by the low percentages in urban areas, especially Addis Ababa. Gambela has the highest percentage of both pregnant teens and teens who have had a live birth - 20.8% and 6.4% respectively - followed by Benishangul and Gumuz. This leaves one in a big conundrum given than Gambela has the lowest fertility of any region in the country. For one reason or another, the early start in childbearing in Gambella does not translate into a higher current fertility (TFR), but Gambella women might still end up with a high number of children ever born (CEB) at the conclusion of their reproductivity, showing the impacts of a disconnect between the "period" effects and "quantum" effects discussed in the fertility chapter.
Contraceptive use
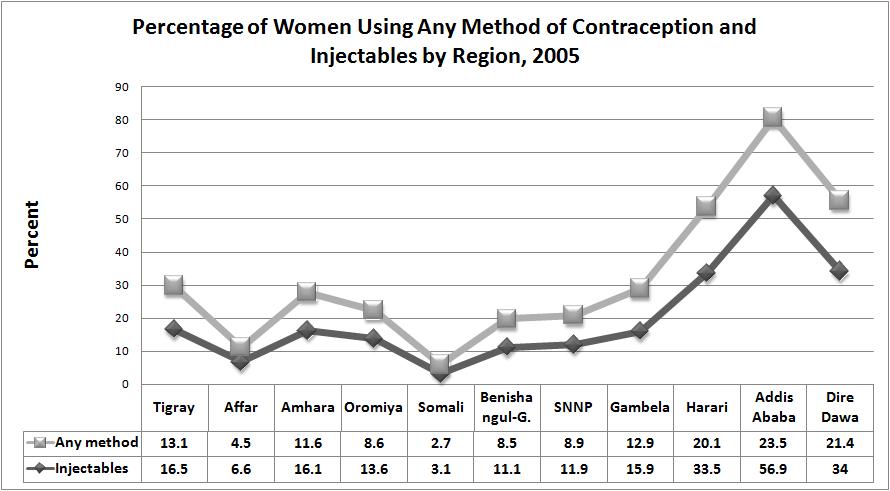
About 15 Percent of Ethiopian women use contraceptives. This is a very low percentage. Contraceptive use rates have climbed in a number of African countries in recent years including Ethiopia itself where the rates were hovering in the low single digits not too long ago. It is 39 percent in Kenya. The rate in Ethiopia is about the same as other countries in the East African region including Djibouti, Rwanda and Mozambique where the level of use has reached 17 percent [8]. The percentage in Oromiya (13.6) is lower than the national average and less than a quarter of the rate in the region with the highest contraceptive prevalence - Addis Ababa. We have added the percentages of women who use injectables in the graph below. Only the urban regions of Addis Ababa, Dire Dawa, and Harari show a significant difference between the percentages using any method and those using injectables, suggesting that almost all of the women in the other regions who use a modern method rely almost exclusively on injectables as a favored contraceptive method. The predominantly nomadic regions of Somali and Afar have the lowest contraceptive prevalence of any region.
Number of co-wives
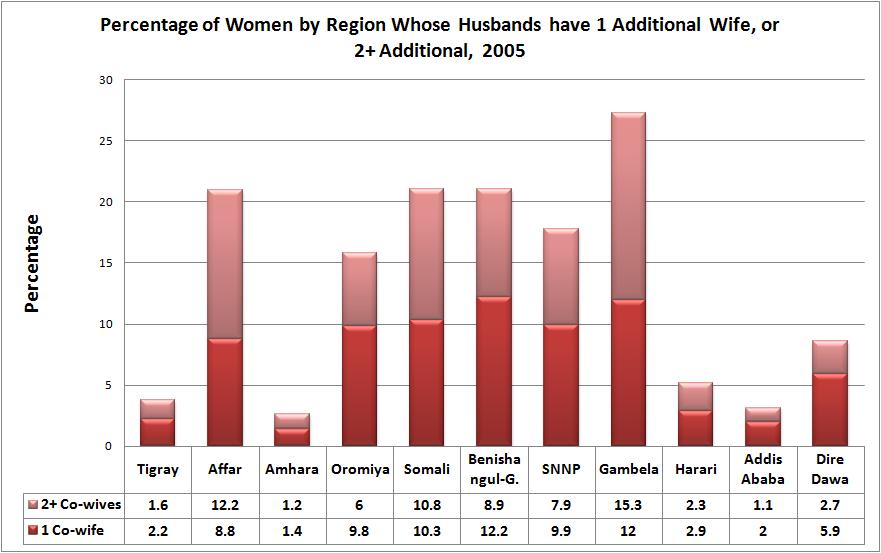
A traditional custom allowing co-wives raises the number of children born to a man (male fertility rates), but can lower the number of children born to a woman (female fertility rate). Popygyny is, therefore, a very useful subject to study. Fortunately, the 2005 DHS included questions and solicited information which allowed the generation of data used in the construction of the graph below. Gambella has the highest polygyny rate with over a quarter of wives sharing their husbands with at least one other wife. Here, the percentage sharing a spouse with two or more wives is actually larger than those with just one other co-wife. One could conclude that after postpartum abstinence (Gambella has by far the longest duration), widespread polygyny is perhaps one of the strongest factors underlying the lowest TFR (in the entire country) of 4.0 observed in Gambella. The nomadic regions of Afar and Somali have almost identical levels of polygyny and the number of co-wives (one, or two or more) shows similar distributions. These two regions are joined by Benishangul and Gumuz for the number 2 status as measured by the prevalence of polygyny in Ethiopia. The prevailing culture and tradition has kept polygyny in Amhara and Tigray at very low levels, even lower than the urban regions of Harari and Dire Dawa.
Postpartum insusceptibility
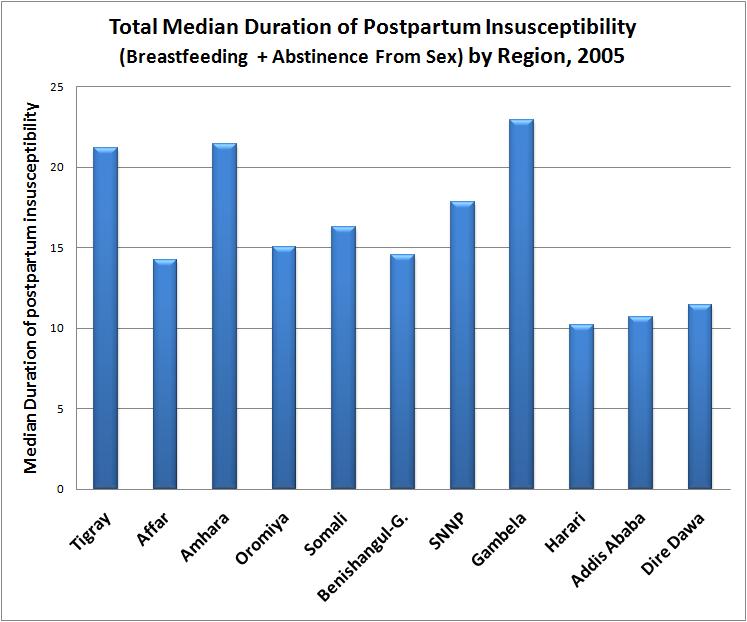
"The duration of amenorrhoea is much shorter among urban women than among rural women, and is lower among women age 15-29, women with secondary and higher education, women in the highest wealth quintile and women residing in Addis Ababa." [7]. The median duration of postpartum amenorrhoea among women in Oromyia is 14. 5 months, one of the lowest in the country and less than the national average of 15.8 months. The overall median duration of postpartum insusceptibility resulting from postpartum amenorrhoea and abstinence from sex in Oromiya is 15. This too is shorter than the national average of 16.7 months. Gambella has the longest median duration of postpartum insusceptibility, a significant contributor being the longest median duration of abstinence from sex in the entire country (11 months) following 17 months of postpartum amenorrhoea. This may be the biggest contributor to the lowest TFR of 4 observed anywhere in the country other than in the predominantly urban regions of Addis Ababa, Dire Dawa, and Harari. Amhara and Tigrean women are a close second with median duration of postpartum insusceptibility of over 21 months. The lowest median duration is in the major cities of Addis Ababa, Dire Dawa, and Harari where a low TFR and sustained decline in fertility over the past years has been driven by factors other than postpartum insusceptibility; namely, contraception, a rise in the marriage age, and a decline in the number of women who would ultimately marry.
Preference for more children
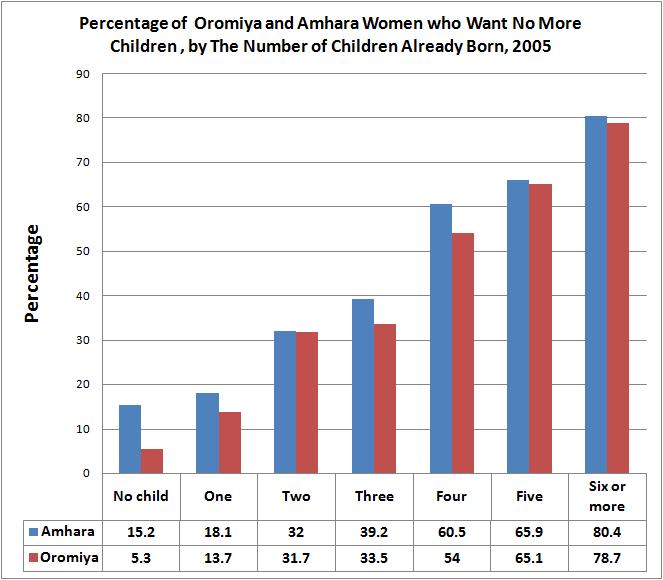
Once again we will use the neighboring region of Amhara for comparative purposes to show preferences among Oromiya women for more children, or lack thereof, based on the number of children they already have (parity). At every parity level, greater percentage of Amhara women than Oromiya women wished to end childbearing altogether. Remarkably, 15.2 percent of Amhara women would like to remain childless. Only 5.3 percent of childless Oromiya women wished to remain in that state. Expectedly, for both Amhara and Oromiya women the desire to have no more children gets stronger with increasing number of children already born. There is a specially significant jump from parity 3 (women with 3 children) to parity 4, with two-thirds as many women who already had four children wanting no more children as women with three children who wanted no more children.
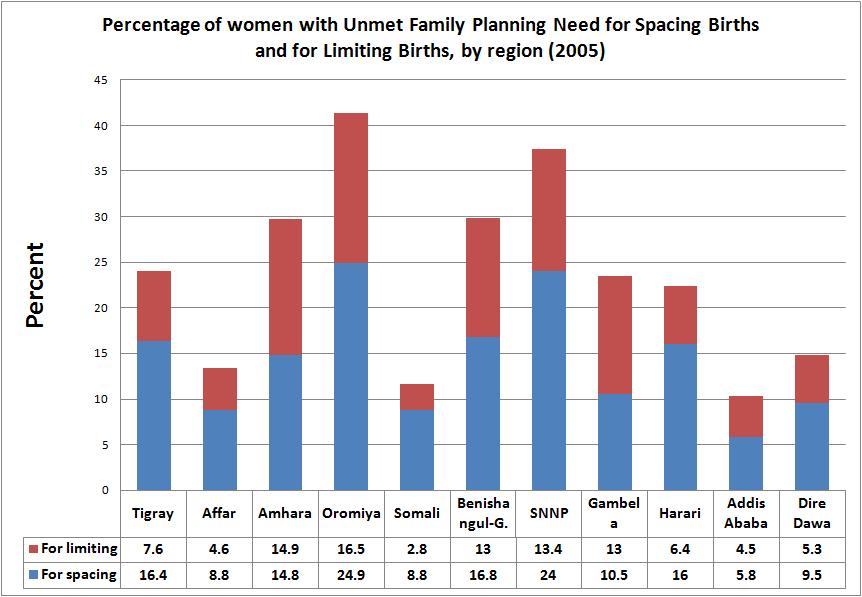
Unmet need for family planning
At 41.4 percent Oromiya has the highest unmet need for family planning. A quarter of Oromiya women would like to have full control over the spacing of births (birth intervals) and another 16 percent would like to stop having children all together. SNNP is a close second, and Amhara and Benishangul-Gumuz third. Nationally, a fifth of the women in their reproductive ages have an unmet need to space births, and 13.7 have an unmet need to stop child-bearing altogether. Given that Oromiya has the highest TFR, it is not surprising that it has the highest unmet need for family planning. Oromiya women asked about their ideal number of children gave responses which showed that the mean ideal number of children (4.2) is two children lower than the actual. "The gap between wanted and observed fertility rates is greater among women living in rural than in urban areas. The difference in the two rates is largest in Oromiya (a two-child difference) and smallest in Addis Ababa" [7].
Administrative map of Oromiya
Childhood Mortality
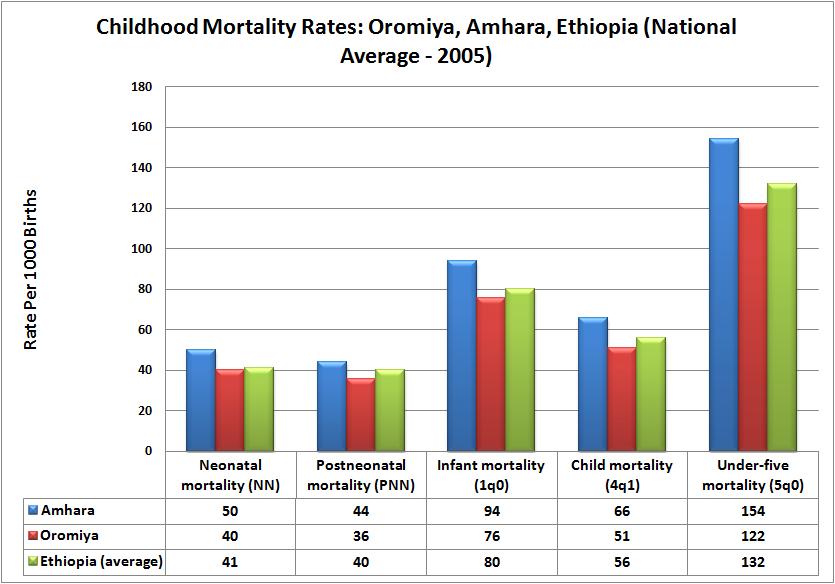
The graph below compares childhood mortality in Oromiya with Amaha as well as the nation at large. A cursory look reveal a clear pattern of a higher mortality in Amhara than the national average, and a lower mortality in Oromiya than the national average. This applies to all four categories of childhood mortality considered. Refer to the mortality chapter for definition of terms like neonatal and postneonatal. Given that childhood health indicators are the best parameters with which social wellbeing is measured, a better showing in Oromiya than Amhara points to a reality of absent socioeconomic advantages accruing to the ordinary Amhara family, and to the fact that past political advantages did not bring the claimed riches and the resulting better health which often accompanies wealth.
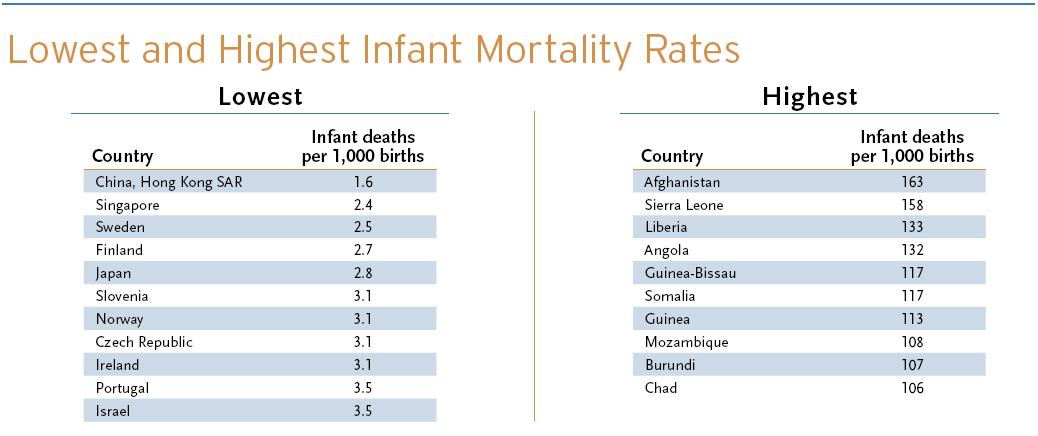
For every 1000 babies born in Amhara, 50 die before turning one month old (10 more than in Oromiya), 44 die between the second and twelfth months (8 more than in Oromiya), giving a total of 94 deaths among Amhara babies before the first birthday (18 more than in Oromiya). The good news is even in Amhara children's survival chances have improved somewhat, and all indications are that childhood mortality will continue to decline everywhere in the country. Just by way of comparison, we have listed (blow the graph) countries around the world with the lowest infant mortality rates, and those with the highest. Compare them with the rate of 80 for Ethiopia and 76 for Oromiya.
Source: [8]
MATERNAL HEALTH
Antenatal care
Antenatal care refers to the care women should receive, but often don't in countries like Ethiopia, before the birth of their child. Care before delivery ideally consists of [9]:
** Pre-conception counseling
** Assessment of risk factors (including maternal health)
** Ongoing assessment of fetal well-being
** Ongoing assessment of complications
** Education about normal discomforts of pregnancy, emotional aspects (including post-natal depression), local antenatal
classes, reducing risk of SIDS, parenting issues (including child-proofing the house and coping with crying infants)
** Discussion of birthing care options
Very few Ethiopian mothers, if any, receive a comprehensive care inclusive of all of these components. The very few mothers who manage to access antenatal care clinics manage to receive just one or two of the above listed care options. In Ethiopia "Twenty-eight percent of mothers received antenatal care from health professionals (doctor, nurse, midwife) for their most recent birth in the five years preceding the survey, and less than 1 percent of mothers received antenatal care from a traditional birth attendant (trained or untrained). More than seven in ten mothers (72 percent) received no antenatal care for births in the preceding five years. Differences in antenatal care by women’s age at birth are not large. Differences by birth order however are more pronounced. Mothers are more likely to receive care from a health professional for first births (34 percent) than for births of order six and higher (22 percent). The use of antenatal care services is strongly related to the mother’s level of education. Women with at least secondary education are more likely to receive antenatal care from a health professional (81 percent) than women with primary education (39 percent) and those with no education (22 percent)." [7]
A quarter of Oromiya women (24.8%) had received antenatal care from a professional care provider. This is a higher than in Somali and Afar, and similar to the rate for Benishangul Gumz. Women in all other regions reported a higher attendance rate of antenatal clinics than women in Oromiya. Expectedly the predominantly urban regions of Addis Ababa (88%), Dire Dawa (52.9%) and Harari (40.7%) had reasonably high attendance rates due to better access to both educational media about the vale of the care and shorter distances and better access to service clinics. Only 3.7% of Oromiya women deliver at a professional health care facility. Over 95% delivered at home with all the attendant risks and complications assisted only by traditional birth attendants (32.5%) and relatives (57.7%). Ethiopian is known to be among countries with very high maternal mortality rate. Eve though specific data on Oromiya are lacking, It would not be a stretch to assume that the grim statistics would apply to Oromiya women too.
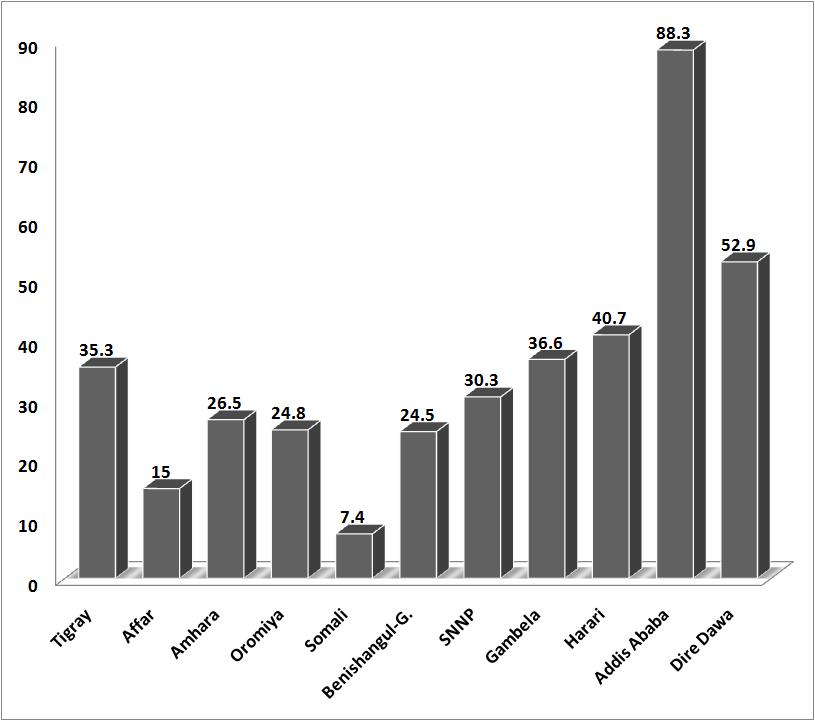
Percentage of Women who had a Live Birth in the Five Years Preceding the 2005 DHS and Received Antenatal Care by Region
A little over 10 percent of Oromiya women who visited the antenatal clinics recived iron tables, 5.3% took intestinal parasitic drugs, 26.1% were informed of signs of pregnancy complications, 75.1% were weighed, 62% had blood pressure measurements taken, 26% gave urine samples, 26.3% gave blood samples [7].
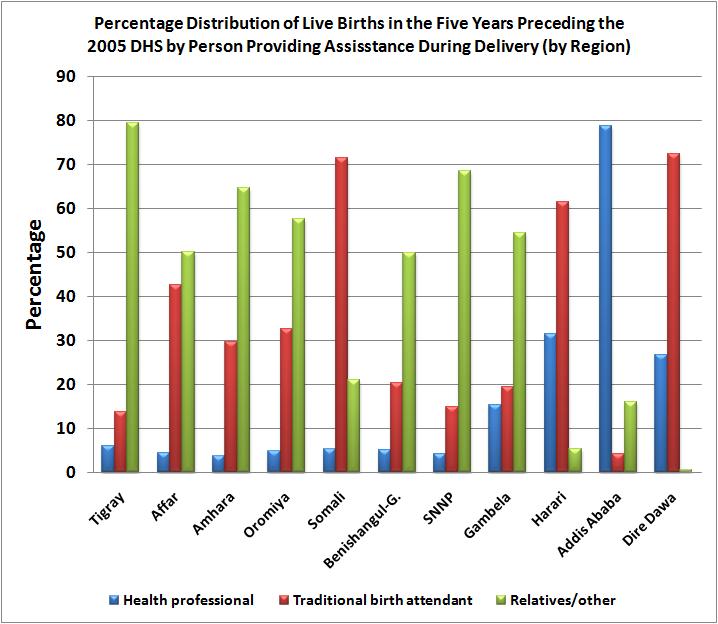
Place of delivery:
Only 3.7% of Oromiya women delivered at a professional health care facility. Over 95% delivered at home with all the attendant risks and complications assisted only by traditional birth attendants (32.5%) and relatives (57.7%). Ethiopian is known to be among countries with very high maternal mortality rate. Eve though specific data on Oromiya are lacking, It would not be a stretch to assume that the grim statistics would apply to Oromiya women too.
The graph below shows percentage distribution of live births in the five years preceding 2005 Demographic and Health Survey (DHS) by person providing assistance during delivery. Two words come to mind in efforts to explain the regional differences the reader sees when looking at the graph especially in the eight non-urban regions of Amhara, Oromiya, Tigray, Gambella, Somali, and Benishangul-Gumuz: culture and tradition. How else can one explain the percentages of 6:1 ratio of Tigrean women who opted for a realtives hand in help to traditional birth attendants, or the 3:1 ratio of Somali women who chose the opposite, favoring traditional birth attendants over relatives. Urbanism has distorted the picture in the urban regions of Addis Ababa, Dire Dawa, and Harari, and has diluted the impacts of culture and tradition when it comes to the use of modern health care, but still 73% of women in Dire Dawa, and 62% in Harari chose traditional birth attendants. Expectedly, the capital city, Addis Ababa has by far the largest proportion of women delivering their babies in a modern health care facility.
Child health
The 2005 DH study in Oromiya also covered "treatment practices and contact with health services among children with the three most
important childhood illnesses (acute respiratory infection, fever, and diarrhea) help in the assessment of national programmes aimed at reducing the mortality impact of these illnesses". Information was also sought on the prevalence and treatment of acute respiratory infections (ARI) and its treatment with antibiotics as well as the prevalence of fever and its treatment with antimalarial drugs and antibiotics. "The treatment of diarrhea disease with oral rehydration therapy (including increased fluids) aids in the assessment of programmes that recommend such treatment. Because appropriate sanitary practices can help prevent and reduce the severity of diarrhea disease, information is also provided on the manner of disposing of children’s faecal matter." Data was also collected regarding a child's wight at birth because "a child’s birth weight or size at birth is an important indicator of the child’s vulnerability to
the risk of childhood illnesses and the chances of survival." [7] Three quarters of Oromiya women described their baby as having average or above average weight at the time of birth. Just over 14 percent of Oromiya children under five were described as suffering from ARI in the two weeks preceding the 2005 survey, 19 percent had fever, and 17.7 percent had diarrhea.
Prevention in the form of vaccines has revolutionized child survival chances in the developed world but only 20.2 of Oromiya children under five years of age had received all of the required vaccinations at the time of the 2005 DHS. Over a quarter of the children received no vaccination at all. The national averages of children who received all of the required vaccines and those who received none was 20.4 and 20 percent respectively.
Persons per sq. km.
Persons per sq. km.
Population Size of Weredas (2008)
Persons per sq. km.
If you would like to help update this page, please send comments and/or data (as an e-mail attachment) to Dr. Aynalem Adugna
at aynalemadugna@aol.com. Don't forget to indicate sources.
Thanks for visiting.
You are visitor number